
tr
Every day between 40 and 60 hairs fall from our heads, and as many are born. It is the natural balance of hair loss in people. But when a person suffers from alopecia they lose that balance and more fall than are born.
Androgenic alopecia, better known as baldness, is not a disease, and it is produced mainly by two causes:
Heredity: Which means that a person, before being born, has already determined in their genetic code whether or not they will have baldness.
Excess sensitivity to male hormones (androgens) by the hormonal receptors of the hair follicles.
Neither stress, nor the use of helmets, nor frequent washing produce baldness. Only on the back and side of the head will they ever fall off, because they are genetically programmed to grow throughout life.
Hair transplantation is a systematic redistribution of hair follicles that consists of the introduction of small scalp grafts that contain so-called follicular units (groups of 1, 2 or 3 hair follicles as they are determined naturally). Each follicle will give a hair. These grafts are obtained from the posterior and / or lateral area of the scalp (donor area) with local anesthesia and, after preparing them under the microscope, they are carefully inserted through micro-incisions in bald areas or areas with little hair that would evolve towards baldness (areas receivers).
By obtaining the grafts from the posterior and lateral areas of the head, genetically programmed to grow throughout life by having hormonal receptors that are not affected by enzymatic hyperactivity, it is achieved that once grafted in other areas they do not fall and continue to grow normally .



Days before the procedure, a medical history is taken, in which the possible causes of alopecia are assessed, and an exhaustive examination of the patient, carefully observing both the area that can be transplanted and the donor area, in terms of density, elasticity , hair color and caliber. Hair implantation lines are studied, for this purpose it is convenient that the patient comes provided with photographs showing their original implantation line. The patient is discussed and advised about their goals and expectations, doubts are clarified, the procedure and postoperative are explained in detail.
Finally, photographs are taken to be able to study the specific case in detail.
Citation
Initial interview with the patient to confirm the agreed objectives and expectations, and clarify existing doubts.
The patient must go to the center at 7.30 in the morning (fasting).
Design of the recipient and donor areas. Only the hair in the area of the donor area that will be resected is shaved, the rest of the hair will remain the same length, in this way the posterior suture will be completely hidden.
Anesthesia
Anesthesia (30 min.)
The anesthetist administers a mild tranquilizer to minimize possible anxiety or nervousness in the patient, avoid discomfort, and prevent any adverse effects caused by local anesthesia.
The donor and recipient areas are locally anesthetized to avoid the sensation of pain and stinging and to prevent postoperative edema (inflammation).
Obtaining the donor area and closing
Donor Area (1h.)
The strip that is extracted passes into the hands of the technical team for the preparation of the grafts.
It is then sutured using the Trichophytic Closure technique to produce a practically invisible healing.
Preparation of grafts
The technical team is in charge of making the micro grafts or follicular units (each with one, two, three or four hairs) under a stereoscopic microscope or magnifying glasses conditioned to the diopters of each technician to create a perfect micro graft.
Once the first micro grafts have been made, the surgeon examines them under magnification, observing their characteristics of color, thickness, and size of the graft.
Only the hair from the donor area to be extracted is shaved, leaving it at 1mm, while the rest of the hair will remain the same length, in this way the posterior suture will be completely hidden. The length and width of the area to be excised is determined by the area to be treated, as well as by the density, the caliber of the hair and the elasticity of the scalp. The strip that is extracted passes into the hands of the technical team for its preparation. The Trichophytic suture used at the Center is used to produce an almost undetectable, practically invisible scar, by allowing hair growth through the scar.
In the case of a second or third procedure, the original scar is extracted, always being replaced by the last one, so that only one scar will remain, which with this technique will be imperceptible.
Incisions (1h.)
The surgeon, equipped with magnifying loupes with incorporated light, makes the incisions whose length and width depend on the dimensions of the follicular unit.
When creating the incisions, the surgeon takes into account several factors (direction, angulation, density and caliber of the hair) that will allow to obtain an optimal aesthetic result.
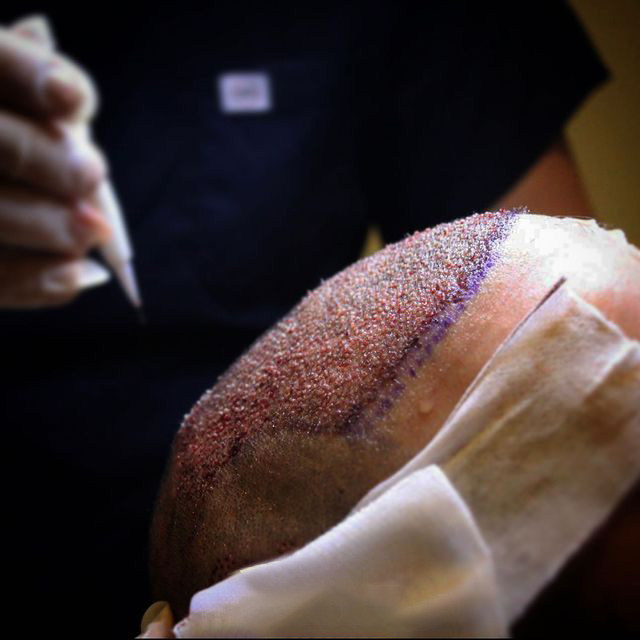
Insertion of grafts (3-4h.)
The insertion of the grafts is carried out taking into account the angles and directions of the insertion sites made by the surgeon. For this, precision tweezers and magnifying glasses are used.
During this time the patient can watch television, can get up to go to the bathroom if necessary or have a snack.
The surgeon, or where appropriate, the team of surgeons, equipped with magnifying loupes (x4.2) with built-in light, then makes multiple incisions whose length and width depend on the length of the specific follicular unit of the patient and the location of the follicular units. In this way, in the first line of implantation, very narrow incisions (0.85mm) are made in which only follicular units of 1 follicle will be inserted, while in the most posterior areas slightly wider incisions (1mm) are made to give room for follicular units of 1,2, 3 and 4 intermixed follicles, thus obtaining a greater density and naturalness.
When making the incisions, the surgeon takes several factors into account: direction, angulation, density (number of incisions per cm2) and the size of the hair to be transplanted. The combination of all these factors in each of the incisions allows to obtain an optimal aesthetic result.
Careful placement of the grafts is performed taking into account the angles and directions of the insertion sites skillfully performed by the surgeon. For this, watchmaker’s tweezers and magnification are used. A follicular unit or micro graft transplant session will provide natural-looking coverage. Future procedures may be performed on previously transplanted areas to increase density if the patient so wishes.
Once all the follicular microunits have been introduced and therefore the transplant is finished, the entire area is carefully cleaned and a woolen cap or cap is placed without any type of bandage.
Finally, the patient is given postoperative instructions by the medical team.
The next day you will go to the consultation to perform the first wash and you will be taught how to do it at home.
During the following days of the week after the transplant, the patient can go to the consultation to perform the washing or it can be done at home.
Approximately 10 days later, you will go to the consultation to carry out the withdrawal of stitches.
Follow-up controls: one month, 3 months, 6 months, 9 months, 12 months and 18 months after transplantation
Evolution
The day after the hair transplant, the recipient area already has small scabs that will come off after approximately 7 days.
During the month following the hair surgery, the implanted hair or hair strand will be lost, maintaining the follicle that will provide new hair.
Around 3 months, the growth of new hair will begin to be seen, although it does not come out all at once.
During the 18 months that follow the Hair Transplant, new hairs will emerge and grow at a speed of 1 cm. a month.
Techniques for obtaining hair follicles
FUSS (Follicular Unit Strip Surgery): A strip 1-1.5 cm wide is obtained for the required length (depending on the density and elasticity) of the posterior and lateral area of the scalp, It is closed with the Trichophytic closure technique. The stitches are removed after 10-12 days.
The strip is processed under the microscope to make the follicular unit grafts by a team of techniques. Allows sessions of up to 4,000 grafts approximately (10,000 hairs)
As a result, a fine scar remains in this area that is aesthetically invisible unless it is shaved to 0, since a change in skin color would be observed.
Prior to transplantation (1 month – 15 days) it is advisable to perform exercises on the scalp to improve elasticity, so practically invisible scars are obtained.
FUE (Follicular Unit Extraction): Using a small punch (cylindrical scalpel) less than 1 mm in diameter, the follicular unit grafts are obtained one by one. It leaves a very small scar in each of the micro incisions that is hardly noticeable even if the patient shaves his head. No need to withdraw points.
The major disadvantage compared to the strip technique is that fewer follicular units (grafts) can be obtained per session (maximum 1,300 – 1,500 follicular units, equivalent to about 3,500 hairs)
Does not require shaving prior to surgery
A greater number of follicular units are obtained.
All grafts are obtained from the “safe” donor area (follicles that will not fall)
The time required for transplantation with the same number of grafts is shortened.
It is the Technique of choice for medium and large sessions (4,000 grafts)
It is cheaper for the same number of follicular units
FUE technical advantages
Multiple imperceptible micro scars that allow zero shaving.
Fast healing that does not require stitches
Very useful technique when there is little elasticity in the donor area.
It is used for sessions with fewer transplanted units.
Who can benefit from an eyebrow transplant?
Men and women who, for certain non-pathological causes (trauma, burn, congenital agenesis …) are missing all or part of the eyebrow.
Cases in which a hair removal has been carried out repeatedly and present very fine eyebrows, or with bald areas.
In cases of basic pathology such as hypothyroidism, universal alopecia, etc. It will be necessary to treat this disease first and assess the response to treatment, once treated it will be possible (if still necessary) to perform an eyebrow transplant.
First, the follicular units of the scalp area are obtained whose consistency is more similar to the consistency of the eyebrow, which are usually temporary areas.
These follicular units can be obtained in 2 ways depending on the number or quantity required:
a- Resecting a small strip of scalp that is subsequently sutured, leaving a scar that is practically invisible (trichophytic technique).
b- Using a 0.8mm diameter punch, which does not require suturing.
In the first case, this strip of follicular units must be subsequently processed by the surgical team to make the grafts.
In the case of having been obtained by means of a punch, these grafts are reviewed and “polished” by the surgical team.
In the case of non-existent eyebrows, a good eyebrow design must be previously carried out, establishing a consensus with the patient.
Since the transplanted hair is hair from the scalp, it has the same characteristics and will therefore grow in the same way, so it must be trimmed periodically as necessary.
The transplanted hair can be treated in any way, that is, dyed, cut, permed, etc., if desired, and always after 2 months.
We do not consider the final result until 16 months have passed after the intervention. During this time, periodic visits should be made to the consultation, mainly in months 1, 4, 8, 12 and 16 after the intervention.
Indications for Eyelash Transplantation:
Total or partial lack of eyelashes, due to trauma, burns, congenital.
Low density
In cases where there is a basic pathology such as trichotillomania, universal alopecia, etc. It will be necessary to treat this disease first and assess the response to the treatment, once treated it will be possible (if still necessary) to perform an eyelash transplant.
First, the follicular units of the scalp area are obtained whose consistency is more similar to the consistency of the eyelashes, although if we compare both consistencies, as a general rule the eyelashes are always somewhat thicker and laminated than the hair on the head. These follicular units should be obtained with long hair (2.5 to 3 cm).
Once the small strip of scalp has been obtained (approximately 3 x 0.5 cm, depending on the density of the donor area), the edges of the wound are sutured using the so-called trichophytic closure, which subsequently allows hair growth through of the scar, so that the scar will go unnoticed.
This procedure is done under local anesthesia.
The strip obtained is divided into follicular grafts of a single hair follicle under a stereomicroscope. The insertion of the follicle in the receiving area is carried out specifically to obtain the typical curvature of the eyelash.
About 25-30 follicular units can be placed per eyelid and procedure. Taking into account that we have approximately 150 lashes per eyelid, this would represent an increase of 20%.
It is advisable to perform a soft permanent eyelash so that they acquire the curvature of the eyelash, as well as other hair treatments such as dyeing, cutting, perming, etc.,
We do not consider the final result until 16 months after the intervention. During this time, periodic visits should be made to the consultation, mainly in months 1, 4, 8, 12 and 16 from the intervention or others whenever you want or need to make a consultation.
